What is Nonossifying Fibroma?
This condition is a benign (noncancerous) and non-aggressive tumor that consists of fibrous tissue. This is considered an indolent tumor meaning that it develops in the bone and grows to a certain size but then stops growing and does not destroy the bone like an active or aggressive benign bone tumor.
Who is usually affected?
- • Twice as likely in males than females.
- • Most common benign bone tumor in children. It is estimated that it is in 20% of children.
Causes
- • There are no known causes of Nonossifying Fibroma.
Diagnosis
- • Imaging includes X-rays, MRI, CT and PET Scans may also be used as well as bone scans.
- • The diagnosis is often confirmed with a biopsy of the bone tumor, which means taking a sample of tumor and having it analyzed under a microscope by a pathologist.
Signs and Symptoms
- • Usually there are no symptoms and it resolves by itself.
- • Patients often injure the area playing sports that leads to identification on an X-ray but its usually not the NOF causing the pain. The pain is usually do to a sprain or strain elsewhere.
Common Bones Involved
- • The most common sites are in the femur and tibia but may occur in the upper extremities.
- • They arise from the part of the bone near the end of the bone called the metaphysis or metadiaphysis as well as toward the perimeter or outer layer of the bone called the cortex.
Biological Behavior
- • Consists of fibrous tissue.
- • An indolent tumor, meaning that it develops in the bone and grows to a certain size but then stops growing.
- • Rarely, an aneurysmal bone cyst, which is a benign aggressive tumor, can develop from an NOF.
Risk to your limbs
Benign (noncancerous) and non-aggressive tumor that consists of fibrous tissue. This is considered an indolent tumor meaning that it develops in the bone and grows to a certain size but then stops growing and does not destroy the bone like an active or aggressive benign bone tumor.
The main risk to the limb is that the tumor grows large enough that it results in a fracture. When it grows to a large enough size it creates a weakness in the bone that the child may break through the bone.
Most however are found incidentally and do not grow large enough to cause a fracture. Very little risk to the limbs as it is usually small heals by itself when the child is fully grown.
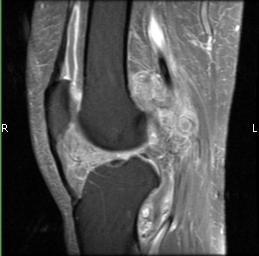
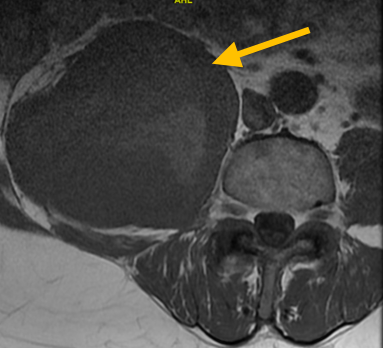
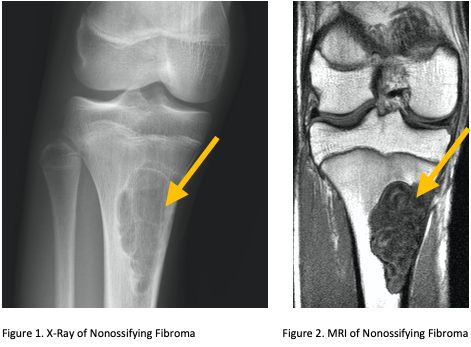
Radiographic imaging is used to help form a diagnosis. These include X-Ray, MRI, CT and Bone Scans.
An example of a X-Ray and MRI are shown.
Treatment of Nonossifying Fibroma
Observation is the most common treatment. In certain cases, surgery should be considered especially if the tumor is large and in young children. Surgical treatments include curettage and bone graft.
Observation

The most common treatment is observation. Nonossifying fibroma most commonly goes away on its own. The bone heals and fills in on its own when the child is fully grown, usually by the age of 21. Observation includes repeat imaging every few months or years to make sure the mass is controlled and the bone is not at risk of being damaged.
Intralesional Curettage
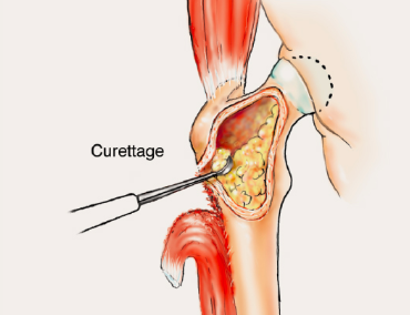
Intralesional Curettage means to scoop the tumor out using a spoon-like tool called a curette. This surgery aims to remove the mass and restore the bone so that the patient can get back to normal function. The mass is identified within the bone and scooped, or curetted, out. The cavity is then shaved down with a Midas Rex Drill, which is similar to a dental drill. This removes more tumor cells.
Bone Grafting and Fixation
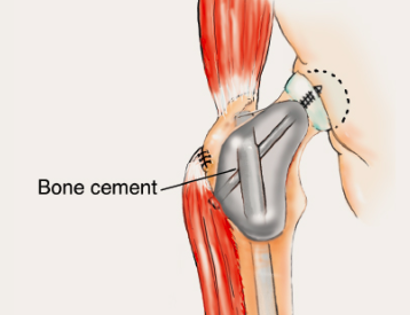
The empty bone cavity is usually filled with bone graft or bone cement. Bone can be donated (allograft) or taken from the patient themselves (autograft). Fixation devices, such as a plate and screws, may be used in specific situations to prevent postoperative fracture.